Home/Resources/Child Welfare/PERSPECTIVES: Breaking New Ground: Massachusetts’ Efforts to Build Diversity-Informed, Reflective, and Relational Infant and Early Childhood Systems

PERSPECTIVES: Breaking New Ground: Massachusetts’ Efforts to Build Diversity-Informed, Reflective, and Relational Infant and Early Childhood Systems

Abstract
Massachusetts has a long history of public–private partnership in infant and early childhood mental health (IECMH) focused on interagency collaboration and investment to advance policy and practice across the commonwealth. One of the primary goals has been to strengthen, diversify, and expand the IECMH workforce across the promotion, prevention, and intervention continuum of care. The Department of Mental Health has made strategic investments to promote access to reflective consultation in partnership with Massachusetts Society for the Prevention of Cruelty to Children (MSPCC) and the Massachusetts Association for Infant Mental Health (MassAIMH). This investment in program leadership and staff has focused on building internal and state capacity in practices that are trauma-responsive, developmentally and relationship-based and culturally humble.
Reflective supervision/consultation (RS/C) is widely recognized as recommended best practice in the provision of infant and early childhood mental health (IECMH) services including, but not limited to, early childhood education, behavioral health, home visiting, pediatrics, and other child and family services. RS/C is a form of ongoing professional development through supervision/consultation and supports practitioners to be able to understand and manage the intense situations and emotions in their work. It affords the provider with time for “stepping back from the immediate intensive experience of hands-on work and taking the time to understand what the experience really means.” (Parlakian, 2001, p. 2)
In the IECMH field, nurturing those who nurture others is important to reduce burnout, increase job satisfaction, and help providers promote high-quality services and positive outcomes in children and families through relationship-based care. However, this relationship-based professional development approach is not easily available for the professionals in the diverse workforce, particularly those not working in a clinical setting. Moreover, diversity-informed RS/C, which invites providers to deepen ways of knowing, being, and doing through critical self-reflection, is particularly difficult to access.
The Massachusetts Department of Mental Health (DMH), through its Children’s Behavioral Health Knowledge Center, has long invested and committed funds to training the children’s mental health clinical workforce in reflective supervision. With the expansion of the state’s IECMH efforts and the Massachusetts Association of Infant Mental Health’s (MassAIMH) adoption of the international credential of Endorsement for Culturally Sensitive, Relationship-Focused Practice Promoting Infant Mental Health® implemented by the Massachusetts Society for the Prevention of Cruelty to Children (MSPCC)/MassAIMH partnership, it became essential to invest specifically in IECMH reflective consultation (RC). A vital expansion in the investment was to increase access to RS/C particularly for professionals of the nonclinical workforce, who play a crucial role in the infant and early childhood system of care.



Strategic Investments in Reflective Consultation
There has been a statewide commitment to operationalize IECMH policies and practices embedded in diversity, equity, and inclusion. Therefore, DMH and other agencies (both private and public) have made strategic investments to promote and expand access to RC in partnership with MSPCC and MassAIMH. Through these collective investments, MSPCC/MassAIMH have offered access to 17 RC groups over 2 years for early childhood professionals in diverse settings statewide. The RC offering is grounded in the Diversity-Informed Tenets for Work With Infants, Children, and Families (Irving Harris Foundation, 2018; see Box 1). Specifically, Tenet #8 (“Allocate Resources to Systems Change”) has focused on building RC capacity for programs and systems across the interdisciplinary early childhood workforce, including offering groups for bilingual bicultural Spanish providers.
Box 1. The Diversity-Informed Tenets for Work With Infants, Children, and Families
- Self-Awareness Leads to Better Services for Families
- Champion Children’s Rights Globally
- Work to Acknowledge Privilege and Combat Discrimination
- Recognize and Respect Non-Dominant Bodies of Knowledge
- Honor Diverse Family Structures
- Understand That Language Can Hurt or Heal
- Support Families in Their Preferred Language
- Allocate Resources to Systems Change
- Make Space and Open Pathways
- Advance Policy That Supports All Families
(Irving Harris Foundation, 2018)
The RC offering promoted essential elements of reflective practice in order to build, sustain, and deepen reflection, with a focus on diversity-informed practice. Another central Tenet in implementation was Tenet #4 (“Recognize and Respect Non-Dominant Bodies of Knowledge”), which operationalized the intentional outreach to engage with professionals with a diversity of race, ethnicity, gender, geography, linguistic ability, and disciplines in mind.
The virtual groups facilitated by MassAIMH Endorsed professionals had 120 providers across diverse settings, including early childhood education, community mental health, pediatric practices, and home visiting. Participants were involved in a year-long collaborative experience of both the “head and heart” of RC, which included didactic training (head) on RC and practice and biweekly group experience (heart) of facilitated RC. Programs that were interested in integrating RC capacity at a programmatic level were offered additional readiness assessment and technical assistance for their leadership teams. The goals of the RC groups were two-fold:
- To support the program leadership and staff workforce through ongoing reflective practice to support skills learned and to strengthen internal capacity for the program in practices that are trauma-responsive, developmentally and relationship-based, and culturally humble.
- To support RC requirements toward MassAIMH Endorsement® requirements for providers.
Evaluation Results
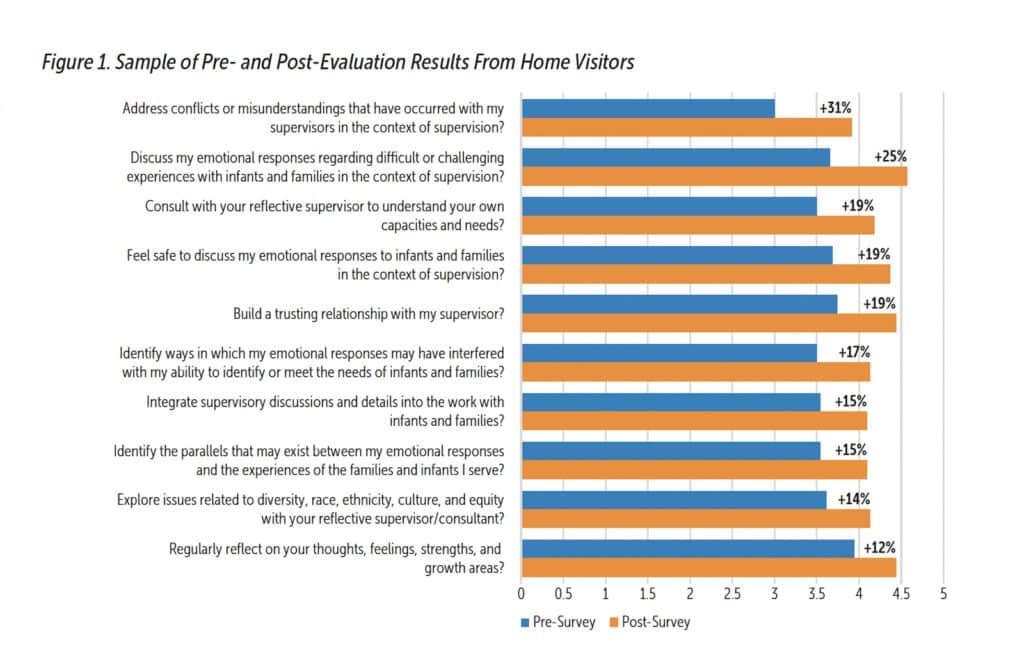
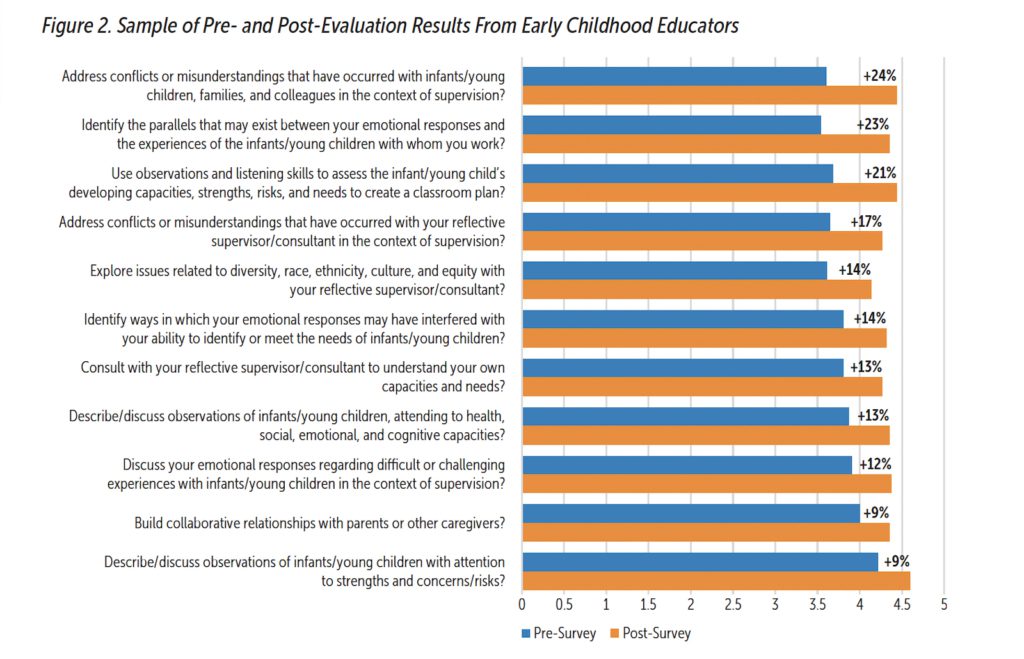
The evaluation of the RC groups included a pre- and post- 28-question survey called the Reflective Supervision Self-Assessment Scales for Home Visitors (Shea et al., 2021) and Reflective Supervision Self-Assessment Scales for Early Childhood Educators (Shea et al., 2019).
In addition, the evaluation included a diversity-informed survey to gather information on how RC invites providers to pay attention to power, privilege, and diversity-informed practice in the context of their work. As seen in Figures 1 and 2, from a sample of the pre- and post-survey on the Reflective Supervision Self-Assessment Scale results, there was an average of 14% increase in providers’ self-efficacy in ability to practice reflectively.
Participants reported a broadened understanding and increased confidence in supporting others through reflection in their own spheres of practice and influence. They also said that the group offering was an opportunity to reflect on their own implicit bias and consider family, context, culture, and language as central to supporting the whole child’s social–emotional and relational well-being. Participants shared the following comments:
The Reflective Consultation group has validated my perceptions of my experience as a supervisor at my current position. This has increased my confidence. It has also given me ideas of how to proceed with supervision in the future, which increased my skills.
The reflective practice group has been an invaluable experience that has allowed me to think deeply about my role as a supervisor. I have learned through listening to colleagues and sharing in a safe and trusted environment that was created by our group leader.
Embodiment and practice of Tenet #1 (“Self-Awareness Leads to Better Service for Families”) in the group reflective experience was elevated through this quote by another participant:
I am learning…not needing to have the answer; being present, actively listening. Not needing to have the answer is what allows for [the creation of] a mutual space.
Learn More
Massachusetts Society for the Prevention of Cruelty to Children. www.mspcc.org/massaimh-endorsement
Massachusetts Association for Infant Mental Health. https://massaimh.org/reflective-supervision/reflective-consultationoffering
Alliance for the Advancement of Infant Mental Health. www.allianceaimh.org
Children’s Behavioral Health Knowledge Center. cbhknowledge.center
The positive results demonstrated in the first round of this RC offering have led to continued investments in funding by DMH and other partners and signal a continued effort to build reflective consultation capacity in IECMH statewide. Furthermore, there continue to be intentional efforts in advancing IECMH professional development, including training in diversity-informed reflective supervision that is grounded in the Diversity-Informed Tenets, that will be offered in the next year by the MSPCC/MassAIMH partnership.
Conclusion
RS/C has been described as a collaborative partnership and relationship for professional growth that enhances program quality and strengthens practice through expanding the capacity of individuals, relationships, and organizations in early childhood work (Shamoon-Shanok, 1991). In Massachusetts, investments in RS/C have become a crucial factor in IECMH workforce development. By providing access to this framework, IECMH training, and scaffolding the professional development of those providing high-quality services for young children and families, the state is not only supporting and growing RS/C capacity, but also building a reflective relational system of care that, in turn, is the foundation for the early relational well-being of young children and families statewide.
Authors
Aditi Subramaniam, LMHC, R-DMT, IECMH-E®, is associate director of infant and early childhood mental health at Massachusetts Society for the Prevention of Cruelty to Children, (MSPCC) a licensed mental health clinician, and registered movement psychotherapist with more than 17 years of experience in the field of mental health, in India and Boston. She leads a statewide workforce development partnership between MSPCC and the Massachusetts Association for Infant Mental Health focused on enhancing, diversifying, and supporting the infant and early childhood mental health workforce with the goal of improving access to services for children from birth to 6 years old and their families. Under her leadership, Ms. Subramaniam collaborates with partners across the state to address gaps and opportunities in workforce needs in the early childhood system to result in better outcomes for all. Ms. Subramaniam is both a clinician at heart and a reflective systems thinker, committed to justice-informed policy, implementation, and practice toward creating equitable systems to meet the needs of Massachusetts’ youngest children and their families. Her clinical experience includes dyadic psychotherapy, community mental health, and home visiting. She is a national trainer for the Newborn Behavior Observation and Brazelton Touchpoints and serves as faculty at the UMass Medical Fellowship on Early Relational Health. She is also a certified DC:0–5TM trainer and is endorsed as an Infant and Early Childhood Mental Health Mentor-Clinical®. She is a ZERO TO THREE Fellow for the cohort of 2022–2024. Ms. Subramaniam has a master’s degree in clinical psychology from Delhi University in India and another in expressive arts and mental health counseling from Lesley University. She has postgraduate certificates in infant-parent mental health and infant observation. The principles and practices of social justice and the arts in psychotherapy are embedded in her everyday work and lens.
Andrea Goncalves Oliveira, MA, IECMH-E®, is infant and early childhood mental health (IECMH) policy and initiatives lead at the Massachusetts Department of Mental Health. Ms. Goncalves Oliveira is a clinical psychologist by training with 15 years of experience working with children and families, both in Portugal and in the United States, in both community and pediatric health settings. She is endorsed as an Early Childhood Mental Health Specialist® and as an Infant Mental Health Mentor–Policy®. Trained in Newborn Behavioral Observation and certified as an infant massage educator and Circle of Security parent educator, her focus has always been on working with and for the youngest children and their caregivers and making a positive impact from the start. In her current role, Ms. Goncalves Oliveira has focused on promoting IECMH awareness across all sectors, educating stakeholders on IECMH policies and bringing public and private partners to the table by breaking down silos and focusing on common goals that will promote well-being for children under 6 years old and their families. She has prioritized investment in workforce development initiatives, including reflective supervision to nonclinical professionals and enhancing early relational health competencies to a diverse group of professionals. As a certified DC:0–5 trainer, she has co-led the expansion of DC:0–5 training statewide, as well as the taskforce that developed the Massachusetts DC:0–5 Crosswalk.
Suggested Citation
Subramaniam, A., & Goncalves Oliveira, A. (2023). PERSPECTIVES: Breaking new ground—Massachusetts’ efforts to build diversity-informed, reflective, and relational infant and early childhood systems. ZERO TO THREE Journal, 43(4), 21-25.
References
Irving Harris Foundation. (2018). Diversity-informed tenets for working with infants, children and families. www.diversityinformedtenets.org
Parlakian, R. (2001). Look, listen, and learn: Reflective supervision and relationship-based work. ZERO TO THREE.
Shahmoon-Shanok, R. (1991). The supervisory relationship: Integrating, resource and guide. ZERO TO THREE Journal, 12(2), 63–76.
Shea, S. E., Goldberg, S., & Weatherston, D. J. (2019). Reflective Supervision Self-Assessment Scales for Early Childhood Educators. [Unpublished measure.]
Shea, S. E., Goldberg, S., & Weatherston, D. J. (2021). Reflective Supervision Self-Assessment Scales for Home Visitors. [Unpublished measure.]
Shea, S. E., Jester, J. M., Huth-Bocks, A. C., Weatherston, D. J., Muzik, M., Rosenblum, K. L., & Michigan Collaborative for Infant Mental Health Research. (2019). Infant mental health home visiting therapists’ reflective supervision self-efficacy in community practice settings. Infant Mental Health Journal, 41(2), 191–205. https://doi.org/10.1002/imhj.21834. https://onlinelibrary.wiley.com/doi/10.1002/imhj.21834